Each mL contains: Haloperidol (as Decanoate) 50 mg.
Haloperidol has a clinical effect which is similar to that of the Promethazines. It has a selective depressant action on the central nervous system. It reduces psychomotor activity, with less sedation than Chlorpromazine. It is anti-emetic. It is used in the treatment of anxiety.
Pharmacology: Pharmacodynamics: Haloperidol suppresses delusions and hallucinations as a direct consequence of blocking dopaminergic signalling in the mesolimbic pathway. The central dopamine blocking effect has activity on the basal ganglia (nigrostriatal bundles). Haloperidol causes efficient psychomotor sedation, which explains the favourable effect on mania and other agitation syndromes.
The activity on the basal ganglia probably underlies the undesirable extrapyramidal motor effects (dystonia, akathisia and parkinsonism).
The antidopaminergic effects of haloperidol on lactotropes in the anterior pituitary explain hyperprolactinaemia due to inhibition of dopamine-mediated tonic inhibition of prolactin secretion.
Pharmacokinetics: Absorption: Administration of haloperidol decanoate as an intramuscular injection results in a slow and sustained release of free haloperidol. The plasma concentrations rise gradually, usually peaking within 3 to 9 days after injection.
Distribution: Haloperidol decanoate is rapidly distributed to various tissues and organs, as indicated by the large volume of distribution (mean values 8 to 21 l/kg after intravenous dosing). Haloperidol crosses the blood-brain barrier easily. It also crosses the placenta and is excreted in breast milk.
Biotransformation: Haloperidol is extensively metabolised in the liver. The main metabolic pathways of haloperidol in humans include glucuronidation, ketone reduction, oxidative N-dealkylation and formation of pyridinium metabolites. The cytochrome P450 enzymes CYP3A4 and CYP2D6 are involved in haloperidol metabolism.
Elimination: The terminal elimination half-life of haloperidol after intramuscular injection with haloperidol decanoate is on average 3 weeks.
Acute and chronic Schizophrenia; Mania and hypomania; Organic psychosis; Agitation in psychotic illness; Explosive hyperexcitability and extreme hyperactivity in children; Motor ties and vocal utterances of Gilles de la Tourette's syndrome; Anxiety neurosis and tension states; Mixed neuroses where features of depression accompany.
The usual intravenous or intramuscular dose is 50 mg, and as rule, can be given more than twice in 24 hours, but this may be increased in accordance with the needs of the patients.
Adults: For rapid emergency control, 1.0 mg will normally be adequate. Up to 30 mg may be given intramuscular injection. Further doses may be repeated every six hours until control is achieved. At any time, oral dosage may be substituted in diminishing doses. The I.V. route may be used if required.
Children: Maintenance dosage: 0.05 mg per kg body weight per day. Where control is not urgent, treatment may be initiated at half the dosage level working up to maintenance dosage.
In general, the symptoms of overdose would be an exaggeration of known pharmacologic effects and adverse reactions, the most prominent of which would be: severe extrapyramidal reactions, hypotension, or sedation. The patient would appear comatose with respiratory depression and hypotension which could be severe enough to produce a shock-like state. The extrapyramidal reactions would be manifested by muscular weakness or rigidity and a generalized or localized tremor, as demonstrated by the akinetic or agitans types, respectively. Since there is no specific antidote, treatment is primarily supportive.
Haloperidol Decanoate (Seredol Deca) is contraindicated in severe toxic central nervous system depression or comatose states from any cause and in individuals who are hypersensitive to this drug or have Parkinson's disease.
Elderly patients with dementia-related psychosis treated with anti-psychotic drugs are at an increased risk of death. Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. Haloperidol Decanoate (Seredol Deca) is not approved for the treatment of patients with dementia-related psychosis.
Avoid to high dosage, since this may cause a variety of minor side effects. Reduce dosage if extrapyramidal dysfunction occurs. Use smaller doses for elderly or debilitated persons.
Pregnancy Category C.
No fetal abnormalities were observed. Haloperidol Decanoate (Seredol Deca) should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Since haloperidol is excreted in human breast milk, infants should not be nursed during drug treatment with Haloperidol Decanoate (Seredol Deca).
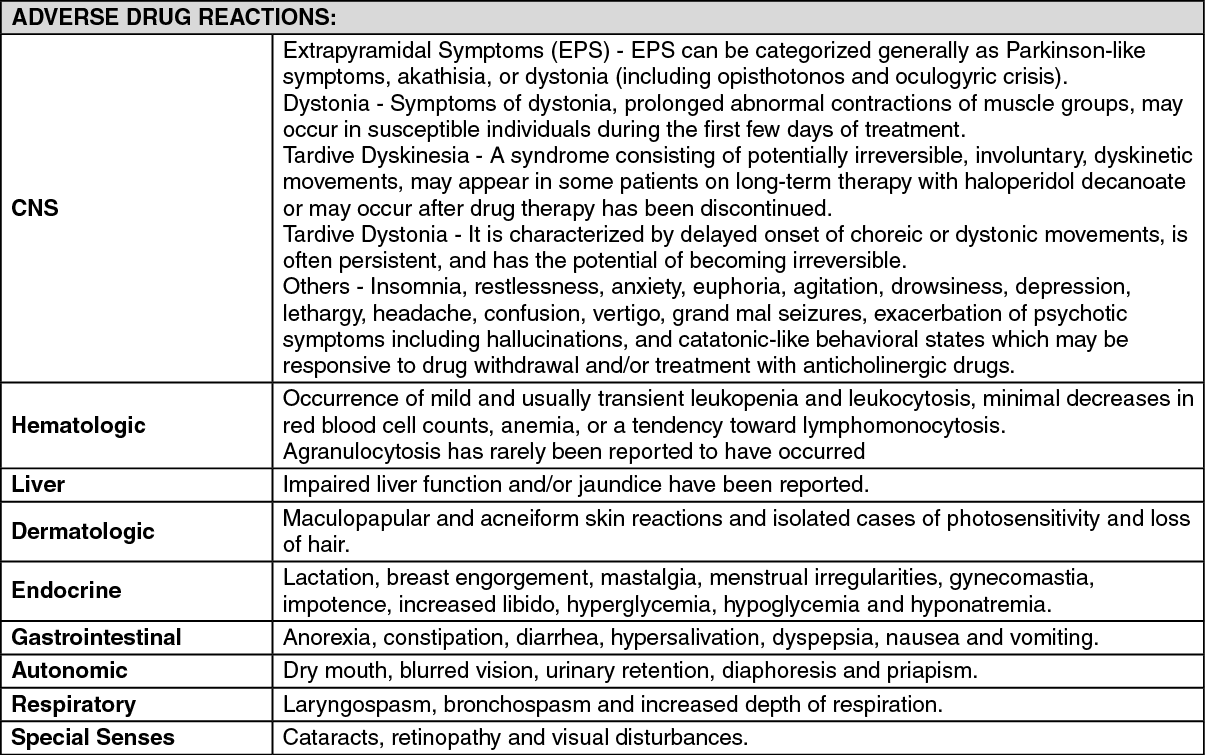
See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Although Haloperidol Decanoate (Seredol Deca) has minimal soporific action, it should be recognized that the drug can potentiate the action of the central nervous system depressants, including alcohol. High doses may potentiate the action of methyldopa as well. As with tranquilizers, it should not be used alone where depression predominates but may be combined with anti-depressants where there is associated anxiety.
Store at temperatures not exceeding 30°C. Protect from light.
N05AD01 - haloperidol ; Belongs to the class of butyrophenone derivatives antipsychotics.
Seredol Deca soln for inj 50 mg/mL
1 mL x 25 × 1's



 Sign Out
Sign Out